 |
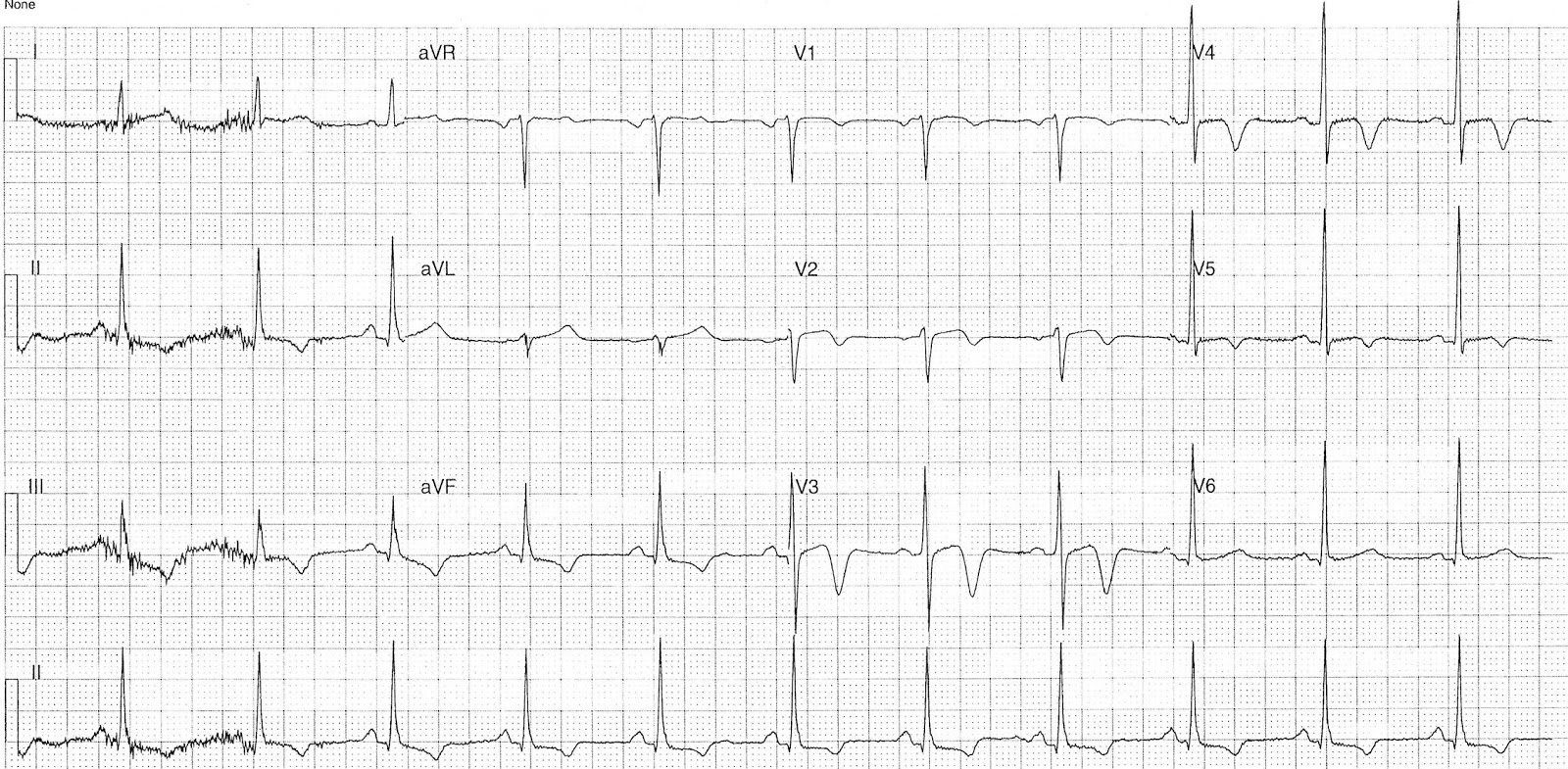
| ECG on presentation Click to enlarge |
- Sinus rhythm, rate 84 bpm
- Normal axis
- Typical LBBB Morphology
- Sgarbossa / Modified Sgarbossa negative
- Isoelectric ST segment in V5 & II
 |
| 15 mins post above ECG Click to enlarge |
Key features:
- Sinus rhythm rate 66bpm
- Normal axis
- Resolution of LBBB morphology
- Narrow QRS
- T wave inversion leads II, III, aVF, V2-5
- Minor up-sloping ST elevation V2-3
- Minor ST depression lead aVF
Interpretation:
- Intermittent LBBB DDx:
- ACS
- Rate related BBB
- Cardiomyopathy
- Myocarditis
- T-wave changes DDx:
- ACS / Reperfusion T waves
- Cardiac T-wave memory
- Cardiomyopathy
- Myocarditis
What happened ?
The patient was admitted under the cardiology team for further investigation. Serial troponin's were negative and the patient under coronary angiogram which showed:
- Right dominant system
- Left main: Normal
- LAD: 30% Proximal stenosis
- Cx: Normal
- RCA: Normal
- Frequent ectopy with mildly impaired LV inferior hypokinesis
Subsequent echo showed:
- Normal LV size and function
- No regional wall motion abnormality
- EF 52%
- Mildly dilated left atrium
- Normal valvular function
He was discharged following above for further out-patient cardiology review.
What is T-wave memory ?
T-wave memory is an interesting phenomenon that could explain the marked T wave changes seen on this ECG. It results in transient T wave changes following a period of abnormal ventricular conduction e.g. ventricular tachycardia, paced rhythms, intermittent bundle branch block or aberrant conduction. There is a recent paper by Vakil that is freely available (linked to below) that contains a nice overview of T-wave memory, proposed mechanisms, and a case example.The deep T wave inversion on this ECG correspond to the leads in which a negative QRS was seen in the patients paced ECG a finding consistent with T-wave memory.
- Vakil K, Gandhi S, Abidi KS, et al. Deep T-Wave Inversions: Cardiac Ischemia or Memory? JCvD 2014;2(2):116-118. Full text here.
References / Further Reading
- Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
No comments:
Post a Comment