At the time of clinical review we luckily had access to her old ECG's and a recent echo.
I plan to include her echo results with the interpretation post although the ECG might give some clues as to the findings.
Check out the original post and comments here.

- Mean ventricular rate ~96 bpm
- Atrial rate ~240 bpm
- Best visualised in lead V1
- Irregular ventricular conduction
- Variable 2:1 & 3:1 conduction
- R - R interval either ~2x or ~3x P-P interval
- Normal (35 deg)
- QRS - Prolonged (~120ms)
- QT - 350ms
- ST depression leads II, aVF, V1-4
- Discordant to QRS vector
- Nil ST elevation
Additional:
- RBBB Morphology
- Significant R' wave V1 ~34mm
- T wave inversion leads III, aVR, V1-4
- Atrial activity
- Best visualised lead V1
- Morphology is same for all complexes
- Isoelectric line is flat
- Unable to visualise in inferior leads
- Atrial tachycardia with variable 2:1 / 3:1 block
- RBBB
- Features suggestive of RVH
- 'Secondary ST / T wave changes right precordial leads a.k.a 'strain pattern'
- Prominent R' wave V1
- Note presence of RBBB complicates the interpretation of ? RVH
Many thanks to Ryan Tee who t has kindly provided a ladder diagram to illustrate the conduction problem seen in this ECG.
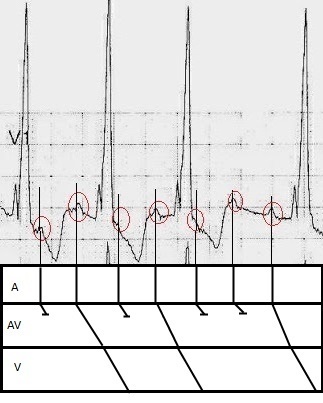 |
| Click to enlarge Image developed by Ryan Tee |
In this case we were lucky to have access to the patient's old notes which revealed the ECG features were old. Her latest echo showed:
- Moderate /Severe Calcific Mitral Stenosis
- Severe Pulmonary Hypertension
- Moderate / Severe Right Ventricular Dysfunction
- Moderate Aortic Stenosis
- Severe Left Atrial Dilation
- Mild Right Atrial Dilation
She was admitted under the medical team for symptomatic treatment of multifactorial dysponea, combination cardiac failure and underlying pulmonary disease exacerbation.
Right Ventricular Hypertrophy on the ECG
There are multiple criteria which may suggest right ventricular hypertrophy (RVH) on the ECG, although it should be noted the ECG has low sensitivity in diagnosing RVH.
The table below is taken from Part V of the freely available AHA series of 'Recommendations for the Standardisation and Interpretation of the Electrocardiogram'(1).
 |
| Click to enlarge RVH Diagnostic Criteria From Ref. 1 |
Also please check out the further reading section for some other relevant blog posts from Life in the Fast Lane and Dr Ken Grauer.
References / Further Reading
Articles
- Hancock EW, Deal BJ, Mirvis DM, Okin P, Kligfield P, Gettes LS, Bailey JJ, Childers R, Gorgels A, Josephson M, Kors JA, Macfarlane P, Mason JW, Pahlm O,Rautaharju PM, Surawicz B, van Herpen G, Wagner GS, Wellens H; American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; American College of Cardiology Foundation; Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part V: electrocardiogram changes associated with cardiac chamber hypertrophy: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol. 2009 Mar 17;53(11):992-1002. PMID: 19281932 Full text here
Life in the Fast Lane
From Dr Ken Grauer
Textbook
- Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
No comments:
Post a Comment