 |
| Click to enlarge |
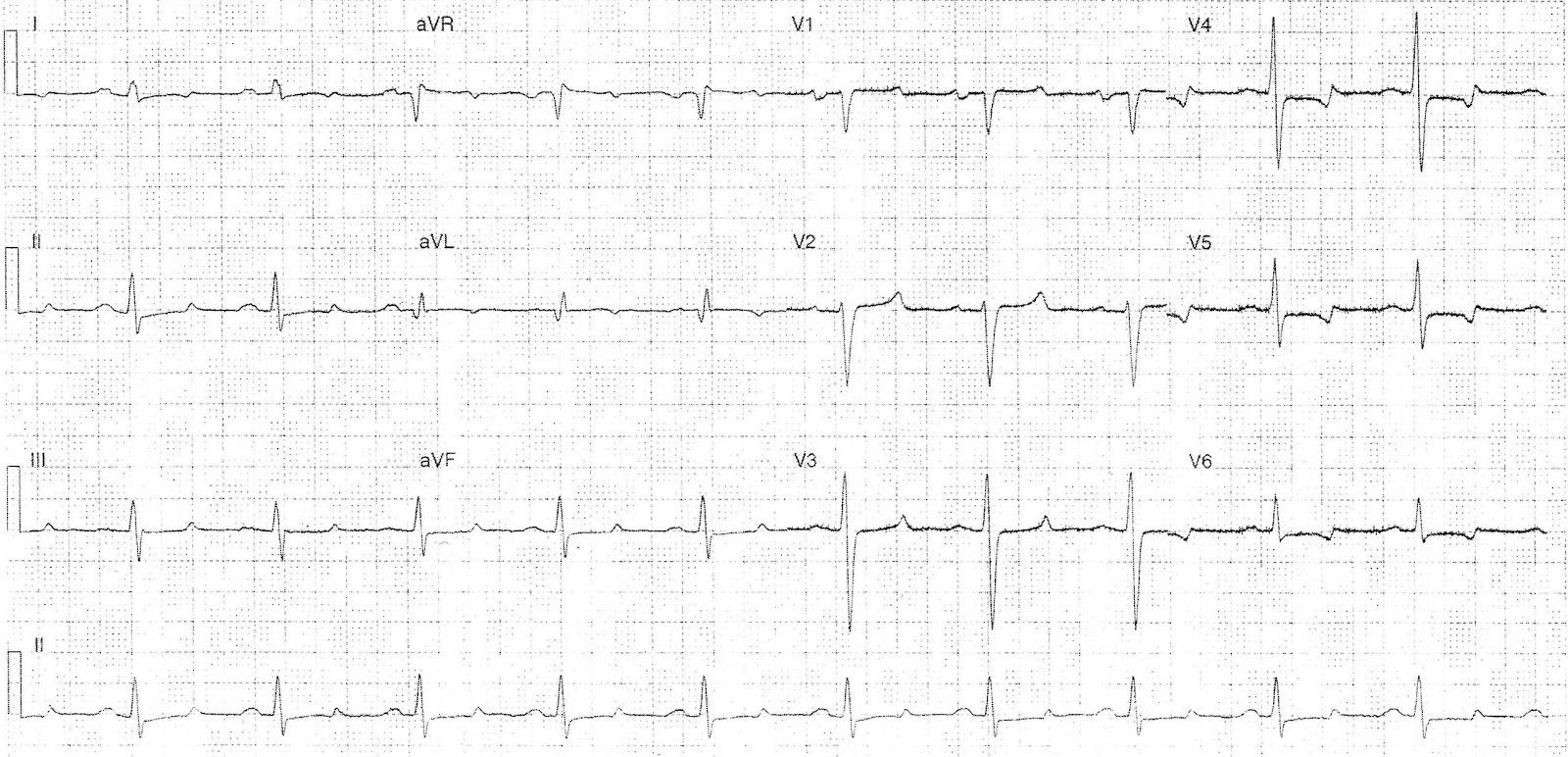
- 60 bpm
- Regular
- Sinus rhythm
- Normal
- PR - Prolonged (~220ms)
- QRS - Prolonged (110ms)
- QT - 480ms
- Note prolonged ST segment with relatively normal size T wave
- Absence of U waves
- Late R wave transition
- Broad P wave in lead II
- ST depression and biphasic (down-up) T wave in leads V4-6
What happened ?
The patient had a corrected calcium of 1.99 (normal 2.2-2.55 mmol/L) and mild hyperkalaemia and hypermagnesaemia.
Classical ECG features of hypocalcaemia are ST segment prolongation resulting in QTc prolongation; there are also reports of T wave flattening and inversion associated with hypocalcaemia, and even ST elevation likely secondary to coronary vasospasm.
The PR prolongation and QRS widening are likely due to the other electrolyte abnormalities, the lateral T inversion may also be due to electrolyte abnormality but serial ECG's, comparison with old ECG's and a focused history exploring potential for other causes (ischaemia, cardiomyopathy, drugs) would be useful to exclude more sinister causes.
Complications of thyroid surgery
- Haematoma / Haemorrhage - Can result in airway compression
- Recurrent laryngeal nerve injury
- Hypocalcaemia secondary iatrogenic hypoparathyroidism
- Infection - superficial / deep
- Seroma
References / Further Reading
Life in the Fast Lane
Textbook
- Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
No comments:
Post a Comment