Pt has a history of congestive cardiac failure, hypertension, hypercholesterolaemia and previous atrial flutter.
Presented with palpitations with no chest pain or SOB when this ECG was taken.
 |
| Click to enlarge |
Rate:
- Ventricular rate ~108 bpm
- Atrial rate ~214 bpm
- Regular
- LAD (-50 deg)
- Apparent PR - Short / Normal (~120ms)
- QRS - Prolonged (140ms)
- QT - 440ms (QTc Bazette ~ 550 ms)
- P Waves superimposed on T waves best seen V1-2
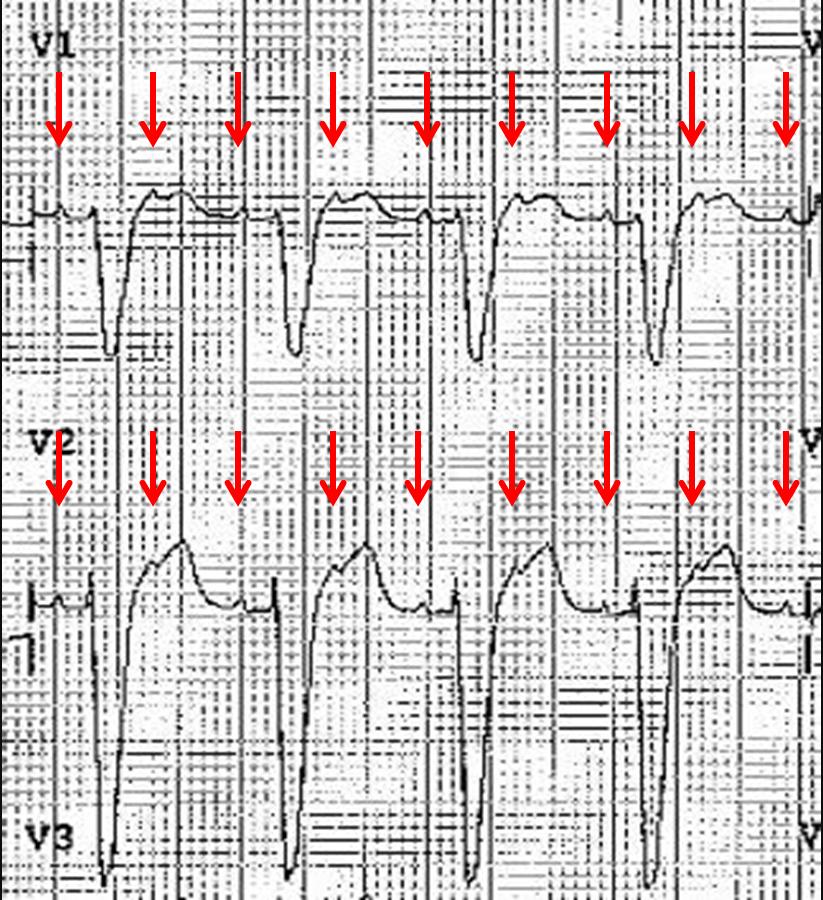 |
| Atrial activity with p waves superimposed in T wave Click to enlarge |
- LBBB Morphology
- Discordant ST Elevation V1-4
- Discordant ST Depression V6
- Atrial Tachycardia
- 2:1 Conduction
- LBBB
- Old in this case
What happened?
The patient spontaneously cardioverted.
Prior echocardiography had shown marked left atrial dilation.
Further episode of atrial tachycardia requiring DC cardioversion.
Underwent left atrial mapping which showed atypical mitral isthmus flutter which was ablated.
References / Further Reading
Life in the Fast Lane
- Atrial tachycardia here
Article - If you want to read a bit about EP studies and differing types of atrial tachycardia
- Saoudi N, Cosio F, Waldo A, Chen SA, Iesaka Y, Lesh M, Saksena S, Salerno J, Schoels W. Classification of atrial flutter and regular atrial tachycardia according to electrophysiologic mechanism and anatomic bases: a statement from a joint expert group from the Working Group of Arrhythmias of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. J Cardiovasc Electrophysiol. 2001 Jul;12(7):852-66. Full text here
- Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
No comments:
Post a Comment